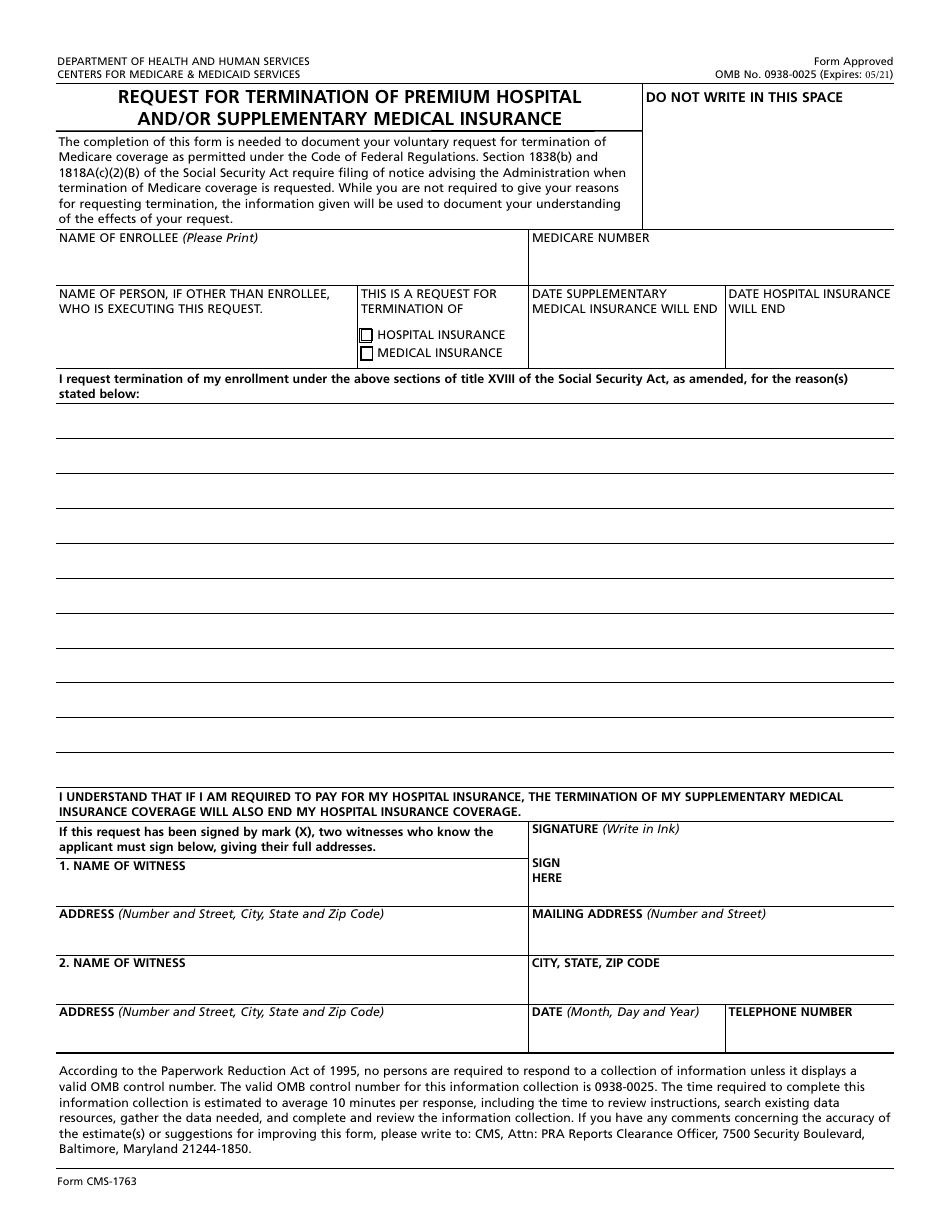
Printable Form Cms 1763 - Web cms 1763 | cms back to cms forms list cms 1763 form # cms 1763 form title request for termination of premium hospital insurance of supplementary. 05/21) request for termination of premium hospital and/or supplementary medical insurance. Web 11 rows cms forms list. The form cannot be completed by cms staff. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Choose the correct version of the editable pdf form from the list and. Save or instantly send your ready documents. Web complete cms 1763 online with us legal forms. Create your cms 1763 in minutes! Web a person who has expressed a wish to stop their medicare coverage will be accountable for paying for their hospital insurance.

Fill Free fillable Form CMS1763 REQUEST FOR TERMINATION OF PREMIUM
Web free cms 1763 template. Select the document or form you need create. Save or instantly send your ready documents. Request for termination of premium hospital insurance of supplementary medical insurance. This is a request for termination of.
1763 form Fill Out and Sign Printable PDF Template signNow
Save or instantly send your ready documents. This request form is the only legal way for a person to terminate their medicare plan a or plan b coverage. At first, seek the “get. Web complete cms 1763 online with us legal forms. Create your cms 1763 in minutes!
Medicare Part B Form Cms 1763 Form Resume Examples X42M4aXaVk
Web cms 1763 printable form. This is a request for termination of. Web 11 rows cms forms list. Web free cms 1763 template. Web find and fill out the correct form 1763.
Social Security Medicare Form Cms 1763 Form Resume Examples wRYPwQW394
Save or instantly send your ready documents. This request form is the only legal way for a person to terminate their medicare plan a or plan b coverage. Web complete cms 1763 online with us legal forms. Customize your document with our simple. This is a request for termination of.
Form CMS1763 Download Fillable PDF or Fill Online Request for
Easily fill out pdf blank, edit, and sign them. Save or instantly send your ready documents. The following provides access and/or. Customize your document with our simple. Web form approved omb no.
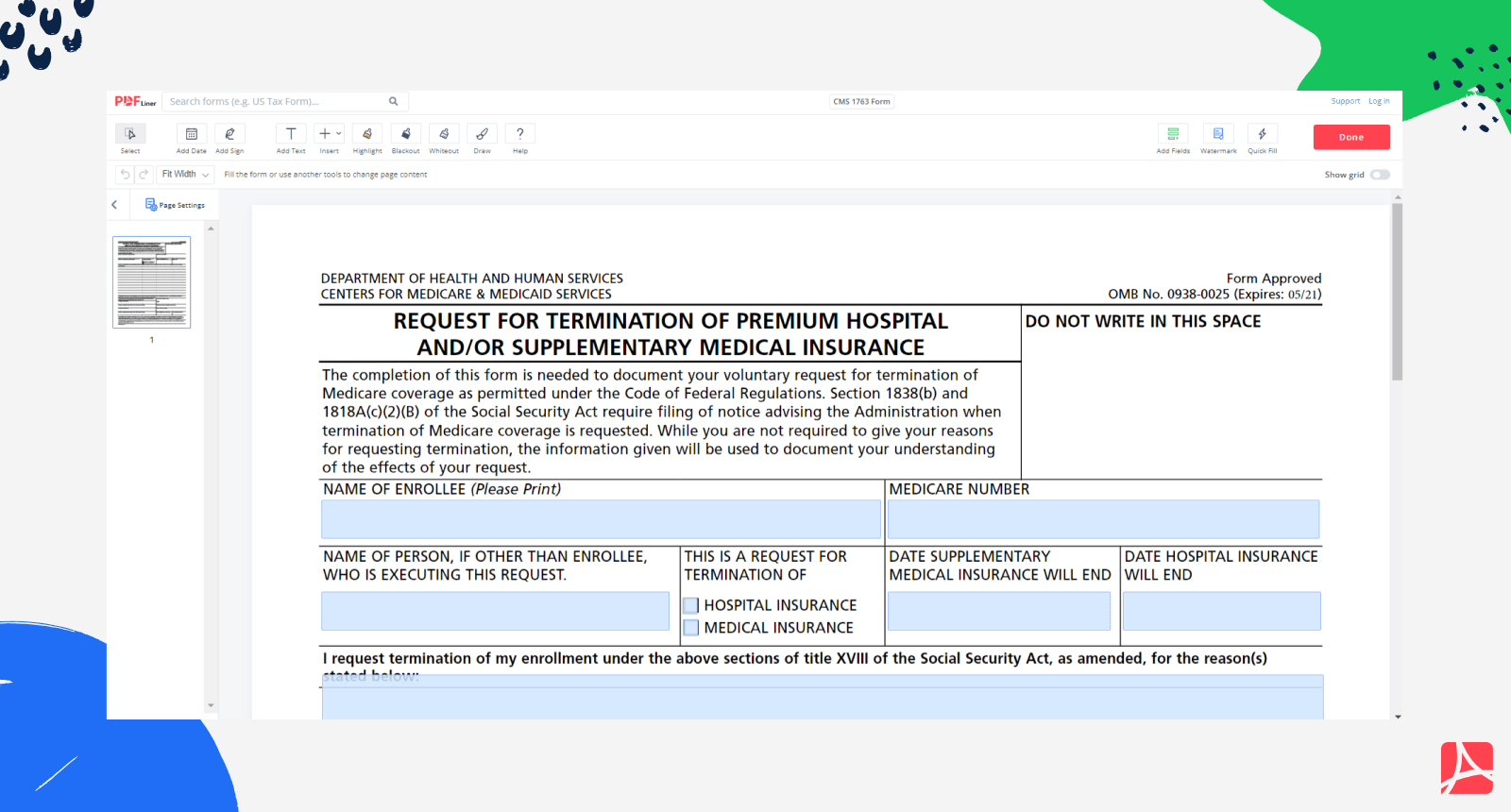
CMS 1763 Form Medicare Form CMS 1763 blank, sign online — PDFliner
Request for termination of premium hospital insurance of supplementary medical insurance. Web complete cms 1763 online with us legal forms. Web 11 rows cms forms list. Department of health and human services. Web watch this video to find out how to terminate premium hospital and/or supplementary medical insurance.

Fill Medicare & Medicaid
Customize your document with our simple. Select the document or form you need create. The form cannot be completed by cms staff. Web 11 rows cms forms list. Web cms 1763 printable form.
Cms 1763 Fillable, Printable PDF Template
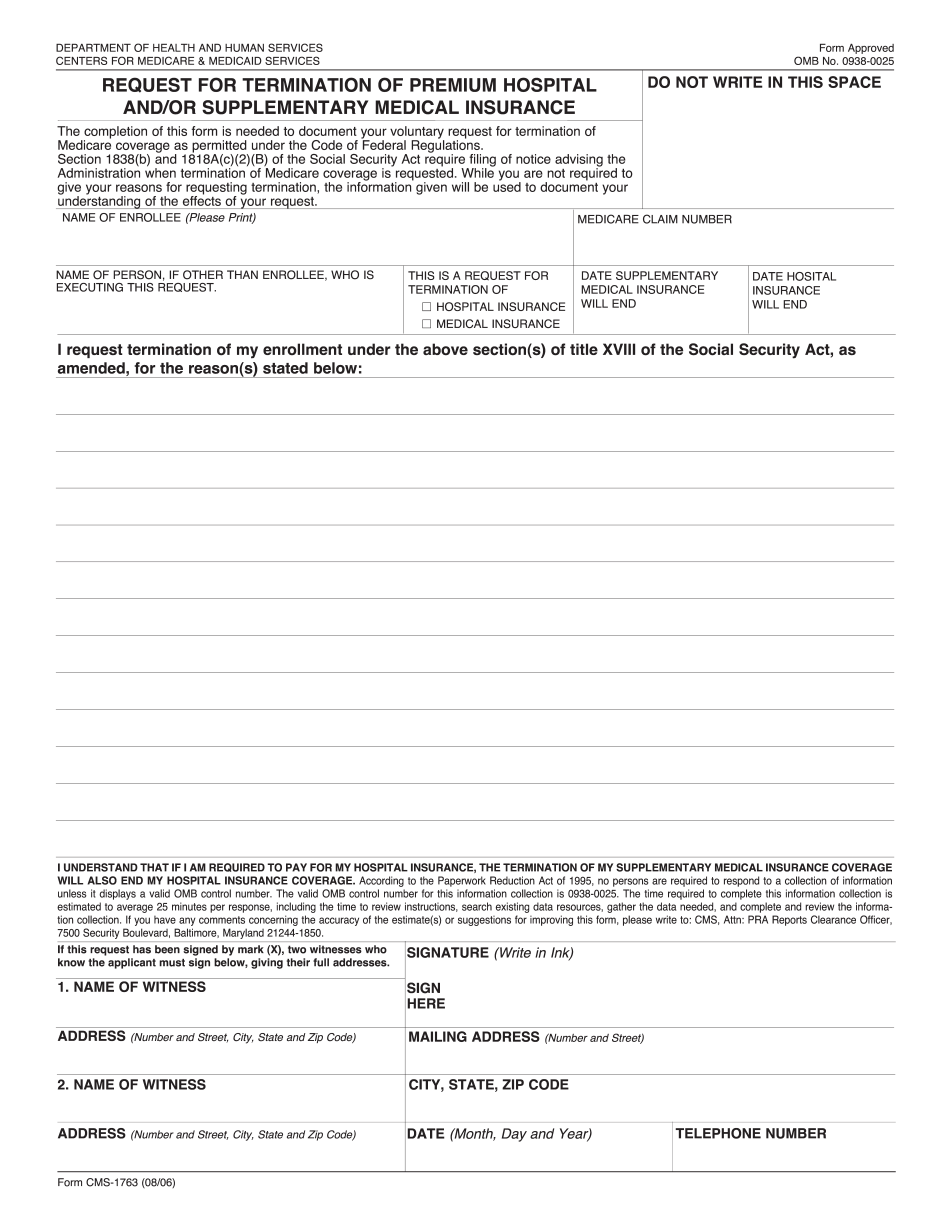
The centers for medicare & medicaid. Web cms 1763 printable form. Web a person who has expressed a wish to stop their medicare coverage will be accountable for paying for their hospital insurance. Save or instantly send your ready documents. Web name of enrollee (please print) medicare claim number name of person, if other than enrollee, who is executing this.

How to fill out CMS Form 1763 YouTube
This is a request for termination of. Web hi 00820.901 exhibit 1: Save or instantly send your ready documents. Web free cms 1763 template. Web 11 rows cms forms list.

CMS 1763 How to opt out of your medicare insurance
Web free cms 1763 template. Choose the correct version of the editable pdf form from the list and. Request for termination of premium hospital insurance of supplementary medical insurance. Web watch this video to find out how to terminate premium hospital and/or supplementary medical insurance. Web 11 rows cms forms list.
Web 11 rows cms forms list. This is a request for termination of. Choose the correct version of the editable pdf form from the list and. Web name of enrollee (please print) medicare claim number name of person, if other than enrollee, who is executing this request. Get everything done in minutes. Easily fill out pdf blank, edit, and sign them. Web cms 1763 | cms back to cms forms list cms 1763 form # cms 1763 form title request for termination of premium hospital insurance of supplementary. This request form is the only legal way for a person to terminate their medicare plan a or plan b coverage. Request for termination of premium hospital insurance of supplementary medical insurance. Web complete cms 1763 online with us legal forms. Save or instantly send your ready documents. Web free cms 1763 template. Web watch this video to find out how to terminate premium hospital and/or supplementary medical insurance. Select the document or form you need create. Web hi 00820.901 exhibit 1: Web a person who has expressed a wish to stop their medicare coverage will be accountable for paying for their hospital insurance. The following provides access and/or. Save or instantly send your ready documents. Easily fill out pdf blank, edit, and sign them. Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s.
Save Or Instantly Send Your Ready Documents.
Request for termination of premium hospital insurance of supplementary medical insurance. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. The form cannot be completed by cms staff. Web watch this video to find out how to terminate premium hospital and/or supplementary medical insurance.
Web Free Cms 1763 Template.
Easily fill out pdf blank, edit, and sign them. Select the document or form you need create. Web name of enrollee (please print) medicare claim number name of person, if other than enrollee, who is executing this request. Web cms 1763 | cms back to cms forms list cms 1763 form # cms 1763 form title request for termination of premium hospital insurance of supplementary.
Save Or Instantly Send Your Ready Documents.
This request form is the only legal way for a person to terminate their medicare plan a or plan b coverage. Create your cms 1763 in minutes! Web complete cms 1763 online with us legal forms. 05/21) request for termination of premium hospital and/or supplementary medical insurance.
The Following Provides Access And/Or.
Choose the correct version of the editable pdf form from the list and. Department of health and human services. Web a person who has expressed a wish to stop their medicare coverage will be accountable for paying for their hospital insurance. Web find and fill out the correct form 1763.